
Authors: Bonnie H. Lee (BSc, PhD student) and Liisa A.M. Galea (PhD, Graduate Program in Neuroscience, Department of Psychology. Djavad Mowafaghian Centre for Brain Health, University of British Columbia)
Every day we learn more about the novel coronavirus (severed acute respiratory syndrome coronavirus 2: SARS-CoV-2). During these early months of the worldwide outbreak, it has become apparent that although men and women may be similarly susceptible to the virus, males are more likely to become severely ill developing the disease, known as COVID-19 that comes from SARS-CoV-2, and worse, have a higher mortality rate. Both biological (sex) and environmental (let’s loosely think of this as gender) factors likely contribute to this sex bias, although most of our focus here will be on the biological contributions.
A research group from China analyzed data from 1099 early cases of COVID-19, including 37 of the first death cases from Wuhan city, and found that in addition to older age and higher number of underlying health conditions, male sex was associated with higher disease severity and mortality rate in patients with COVID-19. Of the 37 death cases, 70.3% were males.
According to Italy’s National Health Institute, 58% of the confirmed novel coronavirus cases, and 70% of the reported deaths from COVID-19 were males. These numbers are consistent with those from China. To date, 25 countries have made data relating to COVID-19 publicly available, but only 6 of them provided the data about both confirmed cases and deaths, broken down by sex: China, France, Germany, Iran, Italy, and South Korea. Through a collaborative effort, CNN and Global Health 50/50 have created a live tracker of the sex-disaggregated data. In order to continue assessing the important differences between males and females regarding COVID-19, it is necessary for all countries to collect and publish their data broken down by sex. Only in this way can we leverage knowledge on sex differences to aid in the discovery of new treatments.
Two ways to approach the sex differences seen with COVID-19 are to examine factors that may cause males to be at greater risk of becoming severely ill with COVID-19 and examine factors that may cause female to be more resilient to becoming severely ill with COVID-19. Both perspectives are needed to understand the differences in mortality rates. In addition, although biological factors like genetics and sex hormones are important to examine, environmental and gendered factors may also contribute to the difference in COVID-19 disease severity and mortality rate between males and females.
Note that the term “sex” is used as a biological variable, defined by the physiological characteristics that define males and females (such as chromosomes, reproductive organs, and sex hormone levels), which is distinct from gender, which involves what a given society may deem appropriate behaviours and activities and/or gender identity (see definitions). It is also important to be aware of the intersectionality between sex and gender.
Biological Factors
Males and females differ in their innate and adaptive immune responses. Typically, females present with stronger immunological responses and are more resistant to virus infections compared to males. Genetically, females possess two X chromosomes whereas males possess one X and one Y sex chromosome, and these chromosomes are present in every cell throughout the body. Interestingly, literature shows that the X chromosome contains many genes that regulate immune function, and it is suggested that because males have fewer of these genes, they are at greater risk of developing certain immune-related diseases. A recent analysis indicates that females had a greater (high range) antibody response when in the severe stage of COVID-19 compared to males. These early analyses suggest some biological component to the sex differences in COIVD-19 responses. Time will tell, with further data, whether this finding is replicated, and whether this effect is seen across age groups.
Sex hormones play an important role in the regulation of the development and function of the immune system. Estrogens, which are produced at higher levels in females, can act by binding to estrogen receptors. Given that estrogen receptors are widely expressed in most cells of the immune system, it is not surprising that estradiol, the most potent form of the estrogens, modulates the functional activity of innate immune cells, and influences downstream adaptive immune responses. On the other hand, androgens, which are at higher levels in males suppress immune cell activity, resulting in inhibited immune reactivity and inflammation. Thus, it is possible that estrogens and androgens play a role in COVID-19 but given that the sex differences are seen in older age groups, which includes postmenopausal females, this suggests that levels of sex hormones can not be the only factor.
Research has identified the angiotensin-converting enzyme 2 (ACE2) as a receptor that is present in many areas of the body including the lungs and nose for the novel coronavirus (Hamming et al., 2004; Xu et al., 2020; Zhou et al., 2020). Data extracted from healthy human lung transplant donors revealed that male donors had higher ACE2-expressing cell ratio, more widespread distribution of ACE2, and a greater variety of different types of cells expressing ACE2, compared to female donors. This suggests that once in contact with the novel coronavirus, the virus has more opportunity to bind with receptors in males compared to females, thus making it easier for the virus to duplicate and potentially cause worse disease outcomes in males. However, we would like to caution that this study only included 8 donors, and only 2 of them were male, and that it will be important in future studies to replicate these intriguing findings. Other research has shown sex differences in ACE2 activity in kidneys, with greater activity in males compared to females that was not dependent on chromosomal sex, but rather 17β-estradiol. Further studies are beginning to bear fruit using gene by sex analyses to examine candidates to combat viral transfer – one such candidate is Muc4, in which expression gives an advantage to female mice but not male mice in viral loads following infection from SARVS-COV.
A study that analyzed lung tissue samples found that smokers (including current and former smokers) had higher ACE2 gene expression compared to non-smokers, even after adjusting for age, sex, and race. More males have reported a history of smoking compared to females according to the WHO, suggesting that males may be predisposed with a higher expression of ACE2 from smoking. In China, sex differences in smoking levels are very high (50% of males and 2% of females are smokers), but the sex difference in Italy is not as profound (28% of males and 19% of females are smokers). Given that both countries show sex differences in mortality from COVID-19 this suggests that sex differences in smoking may contribute but not completely account for the sex differences in mortality rates.
On a related note, it is known that preexisting health conditions confers greater risk for developing a severe case of COVID-19. A report recently released by the Centre for Disease Control and Prevention shows that approximately 80% of ICU and 70% of hospitalized COVID-19 patients in the United States of America reported having at least one underlying health condition. Commonly reported conditions include smoking, lung disease, heart disease, and diabetes. Some of these conditions (mainly lung and heart diseases) are found to be more prevalent among males compared to females. Sex differences in the prevalence of preexisting health conditions may also play a role in the findings that males have a greater morality risk than females from COVID-19.
Environmental Factors
Environmental factors play an impactful role in exposure and infection from viruses. For instance, practicing proper hand hygiene is a crucial for preventing contraction of the novel coronavirus. Curiously, an epidemiological investigation conducted in 2018 found that female participants had significantly greater hand hygiene knowledge compared to their male counterparts. In addition, research shows that females seem to wash their hands more often, use soap more often, and wash their hands for a longer period of time compared to males. And although anecdotal, a recent survey from February 2020 suggests that 65% of females were washing their hands (and keeping surfaces clean) compared to 52% of men surveyed due to coronavirus concerns.
The presence of these different risk and protective factors in males and females may, at least in part, explain the sex differences observed in the disease severity and mortality rate of COVID-19. Moving forward, it remains crucial for research to include and analyze both sexes in their data, so we can further understand the mechanisms driving these sex differences and to propel effective treatments forward for both sexes. It also emphases that the reasons for these sex differences span multiple disciplines and domains and that it will take a concerted effort among a number of different areas of research to fully understand all the factors that contribute to COVID-19 mortality (e.g. social, implementation science, compliance, inflammation, lifestyle choices).
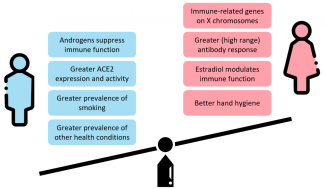
Summary of risk and protective factors in males (blue) and females (pink relating to COVID-19 disease severity and mortality rate.
Lastly, it is important to remember that although mortality from COVID-19 affects men more than women, COVID-19 can affect anyone. Although some may feel as though our risk of becoming sick from the virus is low, there are many younger patients that can have COVID19, and even “mild” symptoms can be devastating. We all need to be doing our part to protect those around us and in the greater community. Let’s continue to wash our hands with soap, stay home, practice physical distancing, and be kind to one another in these trying times.
Bibliography
Bots SH, Peters SAE, Woodward M. Sex differences in coronary heart disease and stroke mortality: a global assessment of the effect of ageing between 1980 and 2010. BMJ Global Health. 2017;2(2):e000298. doi:10.1136/bmjgh-2017-000298
Borchgrevink CP, Cha J, Kim S. Hand Washing Practices in a College Town Environment. Journal of Environmental Health. 2013;75(8):7.
Bouman A, Heineman MJ, Faas MM. Sex hormones and the immune response in humans. Hum Reprod Update. 2005;11(4):411-423. doi:10.1093/humupd/dmi008
Cai G. Bulk and single-cell transcriptomics identify tobacco-use disparity in lung gene expression of ACE2, the receptor of 2019-nCov. medRxiv. February 2020:2020.02.05.20020107. doi:10.1101/2020.02.05.20020107
COVID-19 – Global Health 50/50. https://globalhealth5050.org/covid19/. Accessed March 30, 2020.
Gubbels Bupp MR, Jorgensen TN. Androgen-Induced Immunosuppression. Front Immunol. 2018;9. doi:10.3389/fimmu.2018.00794
Hamming I, Timens W, Bulthuis MLC, Lely AT, Navis GJ, Goor H van. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. The Journal of Pathology. 2004;203(2):631-637. doi:10.1002/path.1570
Jin J-M, Bai P, He W, et al. Gender differences in patients with COVID-19: Focus on severity and mortality. medRxiv. March 2020:2020.02.23.20026864. doi:10.1101/2020.02.23.20026864
Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626-638. doi:10.1038/nri.2016.90
Liu J, Ji H, Zheng W, et al. Sex differences in renal angiotensin converting enzyme 2 (ACE2) activity are 17β-oestradiol-dependent and sex chromosome-independent. Biology of Sex Differences. 2010;1(1):6. doi:10.1186/2042-6410-1-6
Moulton VR. Sex Hormones in Acquired Immunity and Autoimmune Disease. Front Immunol. 2018;9. doi:10.3389/fimmu.2018.02279
Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507-1514. doi:10.2147/COPD.S146390
Plante JA, Plante KS, Gralinski LE, et al. Mucin 4 Protects Female Mice from Coronavirus Pathogenesis. Microbiology; 2020. doi:10.1101/2020.02.19.957118
Schurz H, Salie M, Tromp G, Hoal EG, Kinnear CJ, Möller M. The X chromosome and sex-specific effects in infectious disease susceptibility. Hum Genomics. 2019;13(1):2. doi:10.1186/s40246-018-0185-z
Suen LKP, So ZYY, Yeung SKW, Lo KYK, Lam SC. Epidemiological investigation on hand hygiene knowledge and behaviour: a cross-sectional study on gender disparity. BMC Public Health. 2019;19. doi:10.1186/s12889-019-6705-5
WHO. Who global report on trends in prevalence of tobacco smoking 2000-2025, second edition. Geneva: World Health Organisation; 2018.
Xu X, Chen P, Wang J, et al. Evolution of the novel coronavirus from the ongoing Wuhan outbreak and modeling of its spike protein for risk of human transmission. Sci China Life Sci. 2020;63(3):457-460. doi:10.1007/s11427-020-1637-5
Zeng F, Dai C, Cai P, et al. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: a possible reason underlying different outcome between gender. medRxiv. March 2020:2020.03.26.20040709. doi:10.1101/2020.03.26.20040709
Zhao Y, Zhao Z, Wang Y, Zhou Y, Ma Y, Zuo W. Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCov. bioRxiv. January 2020:2020.01.26.919985. doi:10.1101/2020.01.26.919985
Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270-273. doi:10.1038/s41586-020-2012-7