
Authors: Tori N.Stranges, MPK, B.Kin, PhD Student | Editors: Romina Garcia de leon, Shayda Swann (Blog Coordinators)
Published: May 19th, 2023
It is well understood that sex and gender impacts individual and population health across the lifespan. It is also well understood that marginalized and systemically oppressed groups including women—particularly women of color, Indigenous women, disabled women, and immigrant women, as well as members of the Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer or Questioning, Intersex, and Asexual (2S/LGBTQIA+) community—face health disparities when accessing health care in Canada. Differences exist in disease manifestation, diagnosis time, misdiagnosis, treatment efficacy, and progression of disease resulting in devastating health effects in these populations.
These disparities can be partially attributed to the lack of funding for women’s and 2S/LGBTQIA+ specific health. Studying sex and gender influences is only one step in understanding why health disparities exist across sex or gender. Gender identity and sexual orientation are also key considerations for health research from a health equity lens. The large knowledge gaps in the health of these populations has prompted the Canadian Institutes of Health Research (CIHR) to mandate the incorporation of sex and gender into research. First by recommending the inclusion of Sex and Gender-based Analysis (SGBA) in project proposals in 2010 and then by mandating the incorporation of SGBA into grant proposals in 2019.
A group of recent grads and current grad students (including Tori Stranges, Amanda Namchuk & Tallinn Splinter) were curious how these changes in SGBA resulted in increased mention of sex or gender in funded research proposals. With the leadership of Dr. Liisa Galea and the Women’s Health Research Cluster (WHRC), we searched the publicly available database of grant abstracts funded by CIHR. We analyzed the amount of funded research that mentioned sex or gender in the abstract as well as funded grant abstracts that mentioned either female-specific health research or research within the 2S/LGBTQIA+ community.
In total, we reviewed 8,964 Project and Operating grant abstracts awarded from 2009-2020. We found that under 3% of research funded by CIHR explicitly mentioned SGBA, with 1.94% of grants mentioning sex, and 0.66% mentioning gender within their abstracts. As one of the goals of SGBA is to inform on health equity and understudied populations with respect to SGBA, we also found that 5.92% investigated female-specific outcomes, and 0.35% focused on the 2S/LGBTQIA+ community.
So, what does this all really mean? Our findings suggest more work needs to be done to increase researcher utilization of SGBA as well as to advance health equity in research. It is important to highlight that much of the existing work in this field has unfortunately been focused on binary understandings of sex and gender. Looking beyond this narrow focus allows for a more nuanced understanding of complex issues that include multiple perspectives. Although our understanding of the need for, and recognition of, SGBA in research may be improving, it has yet to be translated into increased research focus and funding. The research community needs to acknowledge that for publications, clinical trials, and grant funding applications, SGBA has not been fully realized despite numerous attempts to support its integration.
So, where does this leave us? The hope of SGBA is that widespread adoption of its principles will result in an equitable future for health where female-specific health, 2S/LGBTQIA+ health, racialized, disabled and gendered experiences, and more are considered. Together we have the power to improve health and reduce disparities, one SGBA at a time.
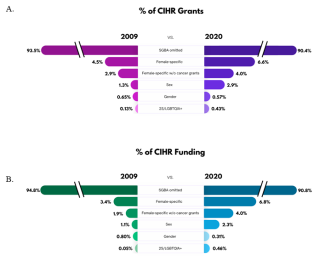
Figure 1: An infographic depicting the change in percentage of grants and funding between 2009 and 2020 for awarded Canadian institutes of Health Research (CIHR) grants for the different categories. The change in percentage (%) of grants (A) and funding amount (B) in the years 2009 and 2020 that “omitted” mention of sex and gender in their grant abstracts or mentioned female-specific health, female-specific health not including cancer based grants, sex, gender, or 2S/LGBTQIA+ health. Reprinted with permission from Stranges et al. 2023
Key Takeaways:
- The percentage of funded grants in which the abstracts mentioned sex or gender in health research remained largely unchanged from 2009 to 2020 with the largest increase of 1.57% for those mentioning sex.
- Total funding amounts for grants that mentioned sex or gender in the abstract stagnated or declined from 2009 to 2020.
- The percentage of funded grants in which the abstracts focusing on female-specific health did not change across 2009-2020, but the percentage of funding dollars increased by 3.47%.
- The percentage of grants in which the abstracts mentioned 2S/LGBTQIA+-specific health more than tripled across 2009-2020 but remained less than 1% of all funded grants.